
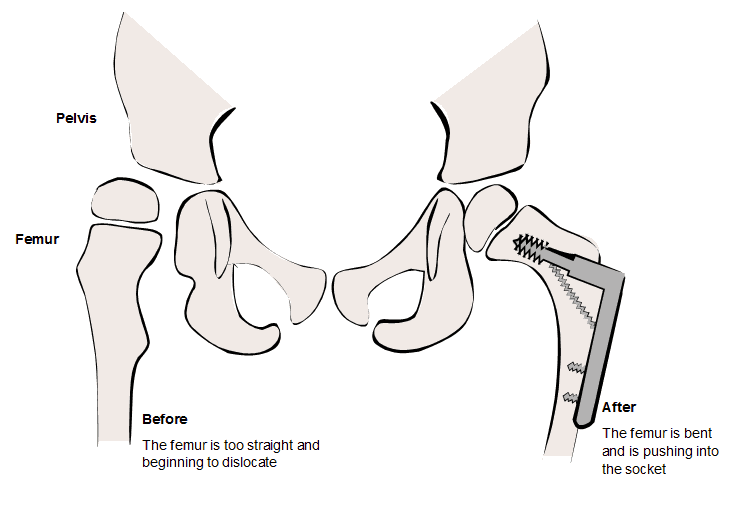
This procedure is often used for correction or prevention of hip dislocation. Children with cerebral palsy are at risk of hip dislocation which can then lead to ongoing hip pain. Hip dislocation will also impact on the ability to sit and stand. This procedure may also be used to correct rotational deformities that affect walking.
The procedure is performed with the child under a general anaesthetic. The surgeon will access the thigh bone (femur) near the hip leaving a vertical scar on the side. A wedge may be taken out of the bone which allows the head of the femur to be angled in and rotated back. To make sure the bones heal correctly, they are held together with metal and screws. This is usually removed one to two years later, well after the bones have healed and strengthened. A plaster cast for the hips (Hip Spica) may also be used to protect the bones. This wraps around the waist and thighs.
Most children will stay in hospital for 5 – 7 days following this surgery, though this may vary. Children are not allowed to weight-bear or stand for 6 weeks after surgery.
Preparation for hospital
Pre-admission clinic
An appointment can be made by the family to see a physiotherapist to discuss how the surgery will affect day to day activities. This appointment can also be used to measure for equipment.
After surgery
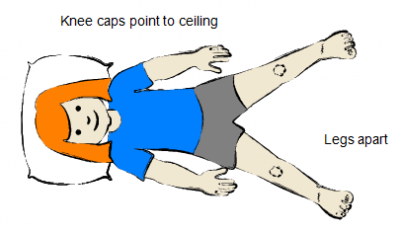
Your child will return from the operating theatre to the ward. The aims at this stage are to manage pain and maintain hip alignment. The ideal position is hips apart with knee caps pointing up to ceiling. Regular change of position is important to avoid pressure sores. Position should be changed every 2-3 hours and the child should be moved carefully to avoid twisting or movement of the hips. Once the child is comfortable and only requires oral medications to sit, lie and change position with or without assistance, they are ready to go home. This is usually 5-7 days but may vary.
Physiotherapy
Physiotherapy can help with positioning and transferring child to and from the wheelchair. Your physiotherapist may be able to start with gentle stretching and moving in the first few weeks. Specific physiotherapy for standing will start when the child is able to weight-bear again, usually at 6 weeks.
Equipment
Your child will need a wheelchair and perhaps a hoist and a commode to help with toileting. Speak to your therapy team for further recommendations and assistance.
Follow up appointments
Your child will need an appointment with your orthopaedic surgeon and an X-ray to check that the bones are healing. The metalwork is able to be removed from the bones once the bones have healed completely. This generally occurs between one and two years post-surgery.
Positioning during non-weight-bearing period
Legs apart
This helps to maintain length in the hip adductor muscles.
The hips should be kept apart when possible, especially when out of the wheelchair. For example, when lying down, knees should be straight. Bring the legs apart slowly. You may be provided with a wedge or brace to maintain this position otherwise towels or pillows can be used to prevent the legs coming together again or the feet rolling in or out. The same approach can be used when sitting on the floor or in a large lounge chair.
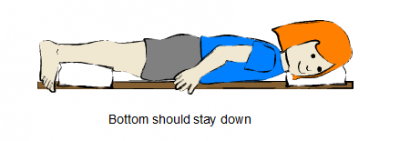
Prone lying
This helps to maintain the length of the hip flexor muscles. Your therapists will advise you if this is an appropriate position for your child post-operatively.
Lie face down and try to keep the bottom down. To prevent the toes becoming too squashed, a pillow should be placed under the shin. Legs should be brought apart slowly as far as possible. This should be comfortable. Reading and drawing can be done in this position. This may be difficult if your child has a Hip Spica. Please talk to your therapy team if you have any concerns.
When to seek help
In an emergency, call Triple Zero (000) and ask for an ambulance.
If you're not sure whether to go to an emergency department, call 13 HEALTH (13 43 25 84) and speak to a registered nurse.
Developed by the Queensland Paediatric Rehabilitation Service, Queensland Children’s Hospital. We acknowledge the input of consumers and carers.
Resource ID: FS190. Reviewed: August 2015.
Disclaimer: This information has been produced by healthcare professionals as a guideline only and is intended to support, not replace, discussion with your child’s doctor or healthcare professionals. Information is updated regularly, so please check you are referring to the most recent version. Seek medical advice, as appropriate, for concerns regarding your child’s health.