
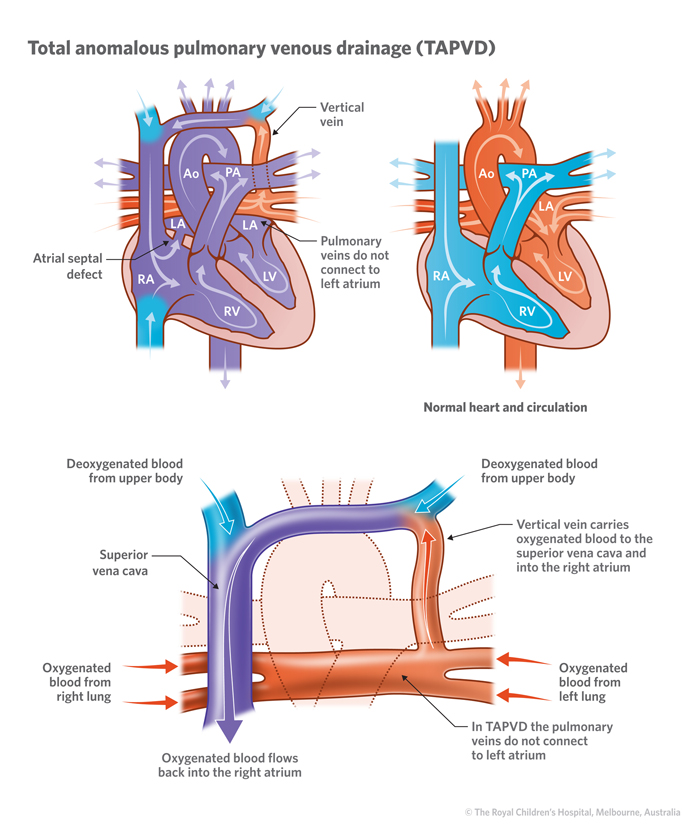
Total anomalous pulmonary venous drainage (TAPVD) is a rare congenital (present at birth) heart defect whereby the pulmonary veins carrying the oxygen-rich (red) blood from the lungs do not connect to the left side of the heart (left atrium). In a normal heart, the four pulmonary connect directly into the heart’s left atrium, enabling the heart to pump the oxygen-rich (red) blood out to the body.
With TAPVD, the pulmonary veins instead, are connected to one of the veins in the main circulation, carrying oxygen-poor (blue) blood and returning to the right side of the heart. This means the red blood simply circles to and from the lungs and never gets out to the body.
Types of TAPVD
There are four types of TAPVD:
Supracardiac
Supracardiac is the most common TAPVD defect. The pulmonary veins drain blood back to the right side of the heart (right atrium) through the superior vena cava. The superior vena cava (SVC) is the large vein that carries deoxygenated “blue” blood back to the right atrium from the upper half of the body.
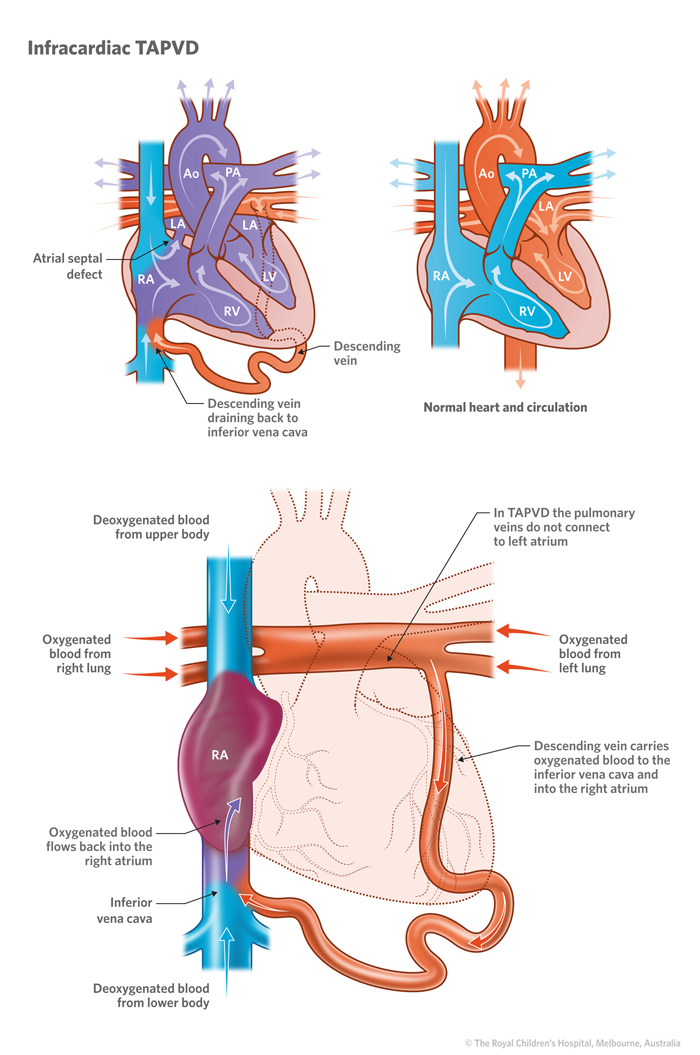
Infracardiac
The pulmonary veins drain into the right atrium through the liver (hepatic) veins and the inferior vena cava (IVC). The inferior vena cava is another large vein that normally carries only deoxygenated blood into the right atrium from the lower half of the body.
Intracardiac
There are two types of intracardiac TAPVD. In one, the pulmonary veins can directly enter into the right side of the heart, into the right atrium. Alternatively, the pulmonary veins can drain into the coronary sinus. The coronary sinus is a vein that normally carries deoxygenated blood from the heart muscle into the right atrium. This vein is usually very small but becomes quite large with this abnormal amount of blood.
Mixed TAPVD
Mixed TAPVD is characterised by the pulmonary veins separating and draining partially to more than one of these above 3 options.
Signs and symptoms
TAPVD is usually diagnosed in the first few months of life, but in some cases, newborns with TAPVD have difficulty breathing and quickly become very ill. This occurs when the pulmonary veins are too narrow or obstructed at some point, and blood can’t flow from the lungs as quickly as it should. This is called TAPVD with pulmonary obstruction. Children with TAPVD with pulmonary obstruction are transferred to intensive care to be stabilized.
Other symptoms in newborn babies:
- Blue skin, lips, and nail beds (cyanosis)
- Rapid breathing (tachypnoea)
- Poor feeding
- Cool, clammy skin to touch
- Lethargy and irritability.
Sometimes TAPVD is diagnosed later. These symptoms are often milder and can include:
- Repeated respiratory tract infections and difficulty breathing
- Heart murmur or cyanosis (blue tint to skin, lips, nail beds)
- Poor feeding, irritability and poor weight gain.
Diagnosis
A diagnosis of TAPVD may be suspected when a doctor hears a typical heart murmur. They may see evidence of overload on the right side of the heart.
Tests such as chest X-rays, electrocardiograms (ECG) and echocardiograms may be used to diagnose TAPVD. Sometimes cardiac catheterisation is needed.
Treatment
Treatment for TAPVD will depend on your child’s age, overall health and the extent of their condition. A child with TAPVD will most likely be admitted to an intensive care unit or a special care nursery for close observation, and may require oxygen and, in some cases, mechanical ventilation (a breathing tube to assist their breathing until surgery).
A cardiac catheter can be used in the initial treatment of some cases with a procedure called a balloon atrial septostomy (BAS). This involves a catheter with a balloon being inserted to enlarge the opening in the wall between the left and right atria to improve the mixing of the blue and red blood to improve oxygenation to the body.
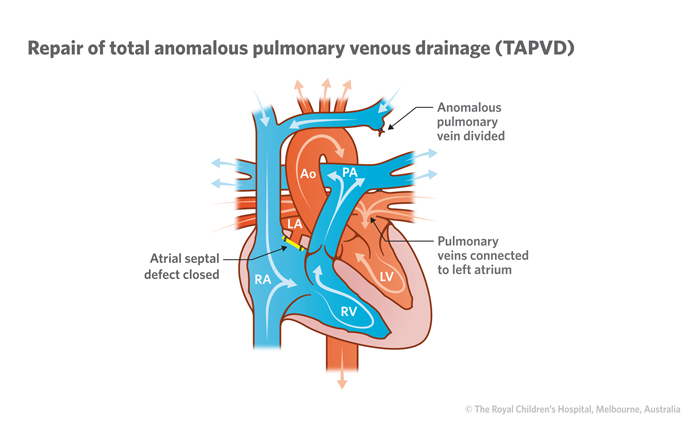
Surgery
Surgery involves reconnecting the four pulmonary veins to the left atrium as well as correcting any other defects present.
Developed by Queensland Paediatric Cardiac Service, Queensland Children's Hospital.
Resource ID: FS241. Reviewed: October 2023. Illustrations courtesy of the Royal Children’s Hospital Melbourne.
Disclaimer: This information has been produced by healthcare professionals as a guideline only and is intended to support, not replace, discussion with your child’s doctor or healthcare professionals. Information is updated regularly, so please check you are referring to the most recent version. Seek medical advice, as appropriate, for concerns regarding your child’s health.