
View resources
Key points
- Consider AOM in any young child who presents with irritability, lethargy, otorrhoea and fever regardless of the presence of localised ear pain.
- Diagnosis is routinely based on symptoms and otoscopy findings.
- Primary treatment is aimed at reducing pain.
Isolated, unilateral AOM usually resolves after two days without antibiotic treatment. - Always consider the possibility of sepsis in an unwell child with a fever.
Purpose
This document provides clinical guidance for all staff involved in the care and management of a child presenting to an Emergency Department (ED) with symptoms of acute otitis media (AOM) in Queensland.
This guideline has been developed by senior ED clinicians and Paediatricians across Queensland, with input from senior staff in Infectious Diseases, ENT and Pharmacy, Queensland Children’s Hospital, Brisbane. It has been endorsed for use across Queensland by the Queensland Emergency Care of Children Working Group in partnership with the Queensland Emergency Department Strategic Advisory Panel and the Healthcare Improvement Unit, Clinical Excellence Queensland.
Introduction
AOM is a rapid onset active infection of the middle ear, characterised by otalgia (earache), irritability and fever.1 It is a common problem with 66% of children reportedly experiencing an infection by three years and 90% by 6 years of age.2,3
The majority of AOM infections have a combination of viral and bacterial aetiology (estimated to be 66% infections). Approximately 27% of infections are solely bacterial and less than 5% are only viral.4,6
AOM is primarily a result of eustachian tube dysfunction. In a viral upper respiratory tract infection, physical and immunologic changes in the nasopharynx allow the normal bacterial colonisers (commonly Streptococcus pneumonia, Haemophilus influenza, and Moraxella catarrhalis) to enter the eustachian tube.3,4 Infants and young children are at greater risk of infection owing to the anatomy of their eustachian tubes (short, wide, straight and in a relatively horizontal plane).5
Risk factors for recurrent infections include:
- exposure to cigarette or wood smoke
- day care attendance
- use of a dummy
- Indigenous or Torres Strait Islander background
- short duration of breastfeeding7,8
Most cases resolve without complications. Tympanic membrane perforation (presenting as pain relieving discharge from ear) is a complication that occurs in approximately 7% of cases.9 Over 90% of perforations heal spontaneously.10 Chronic suppurative otitis media refers to persistent perforation with draining exudate for more than 6 weeks.
Rare but serious complications include:
- mastoiditis
- infection spreads from the middle ear to the nearby mastoid air cells
- estimated incidence of 1: 1,000 AOM cases in developed countries, more common in Indigenous children15
- intracranial complications such as meningitis, brain abscess, subdural empyema14
- caused by direct bacterial invasion from the middle ear and mastoid, or haematogenous spread to the intracranial space
- facial nerve palsy
- occurs in less than 1 per 100, 000 cases11
- sepsis
- lateral sinus thrombosis
Assessment
There is no gold standard for the diagnosis of AOM.1 Pain is the major symptom, but the diagnosis should be considered in any child who presents with irritability, lethargy, otorrhoea and fever, with or without localised ear pain. Infants may present with feeding difficulties.
Do not accept AOM as lone focus of fever in sick febrile child. Always consider the possibility of sepsis.
History
History should include specific information on:
- pain (including location and onset)
- discharge from the ear
- behaviours such as rubbing or tugging at ear
- history of fever
- use of anti-pyretics
- systemic symptoms
- previous ear infections
Examination
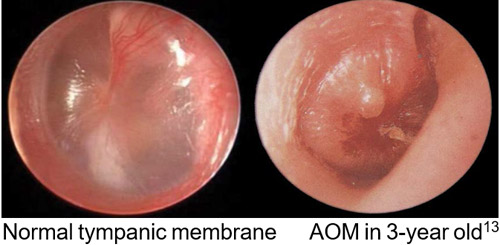
Otoscopy
Otoscopy is the most important examination procedure in the diagnosis of AOM. Parental assistance can help ensure adequate immobilisation of the child and improve visualisation of the tympanic membrane. Most parents feel comfortable holding the child in their arms with the head held resting against the parent’s shoulder or chest and holding the child’s arms.

Assessment of the auditory canal and tympanic membrane includes:
- presence or absence of discharge
- position of tympanic membrane (neutral, retracted or bulging)
- colour
- translucency
- mobility
- perforation
Otitis media with effusion (OME), also known as “glue ear”, is a collection of non-purulent fluid (effusion) in the middle ear. It is usually seen as a result of AOM, is often asymptomatic, and if persists can lead to hearing impairment. Differentiating between AOM and OME can be challenging.
| AOM | OME |
|---|---|
Tympanic membrane is typically:
| Tympanic membrane is typically:
A fluid level or bubbles may be seen behind the tympanic membrane |
Clinical diagnosis of AOM requires ALL of the following
- onset <48 hours
- redness and bulging of the tympanic membrane (middle ear inflammation)
- middle ear effusion
Redness of the tympanic membrane alone is not suggestive of AOM. Redness can also be caused by many other processes including crying, fever, URTI and trauma.
Serious complications of AOM
| Complication | Presentation |
|---|---|
| Mastoiditis | May present with fever, ear pain, retro-auricular swelling and/or erythema with mastoid tenderness. The affected ear may be pushed forward and downward |
| Facial nerve palsy | Unilateral facial droop / lower motor neurone signs |
| Intracranial complications (including meningitis, brain abscess and subdural empyema) | AOM with fever, headache, vomiting, irritability, or altered conscious state, with or without focal neurologic signs14 |
| Sepsis | Toxic features (see Sepsis guideline) |
Investigations
As AOM is a clinical diagnosis, investigations are not routinely recommended.
Tympanocentesis (to obtain middle ear fluid for culture) should only be performed by an ENT surgeon and is usually not required since antibiotic therapy (if indicated) should be started empirically.
Where there is AOM with perforation, a bacterial swab from the ear canal is recommended if there is reason to suspect resistant organisms (e.g. failure of initial antibiotic treatment).
Management
Refer to the flowchart [PDF 261.81 KB]for a summary of the recommended emergency management of a child presenting with symptoms suggestive of AOM.
Refer to the Sepsis guideline for a child with toxic features.
Pain relief
Oral analgesics should be used early to minimise the pain associated with AOM.
| Analgesic | Dose |
|---|---|
| Paracetamol (oral) | Age over three months: 15 mg/kg/dose (maximum 1 g) every four hours, maximum four doses in 24 hours. (Dose based on ideal body weight) |
| Ibuprofen (oral) | Age over three months: 10 mg/kg/dose (maximum 400 mg) every six to eight hours, maximum three doses in 24 hours |
| Oxycodone (oral) | 0.1 mg/kg/dose (maximum 5 mg) orally every four hours when required. Maximum four doses in 24 hours |
Additional relief can be obtained topically, if the tympanic membrane is intact, with Auralgan Ear drops. These are instilled in the ear and plugged with cotton wool. This item is not on LAM but can be obtained in the community.
Antibiotic therapy
Antibiotics do not alter the course for most children with mild, uncomplicated AOM.15 Without antibiotic treatment, pain resolves after 24 hours in 60% of children, and most infections resolve spontaneously within seven days. Evidence suggests that antibiotics may reduce the risk of tympanic membrane perforation or AOM in the contralateral ear, however is associated with side effects including vomiting, diarrhoea and rash. There is insufficient evidence to determine if antibiotic use reduces the risk of mastoiditis or meningitis.15
Antibiotic therapy is not routinely recommended for mild uncomplicated AOM. Consider if symptoms persist after 48 hours. At this time antibiotics may be initiated following clinical review or at the parent’s discretion (if provided with a script at the initial consultation). Evidence suggests relying on parental assessment reduces antibiotic usage by up to two thirds with equivalent parental satisfactions rates when compared to early antibiotic treatment. The Australian Commission on Safety and Quality in Health Care has developed a decision aid for consumers which assists with shared decision making around antibiotics.
Most children with isolated unilateral AOM do not require antibiotic therapy
Consider antibiotic treatment for the following children:
- age less than six months
- age less than two years with bilateral AOM
- symptoms for more than 48 hours
- severe symptoms (fever > 39°C and moderate to severe otalgia)
- evidence of perforation (purulent otorrhoea or perforation visualised)
- higher risk of complications including:
- Indigenous or Torres Strait Islander background
- immunocompromised
- uncertain access to follow-up
Clinicians working in Townsville, Cairns and Gold Coast Hospital and Health Services should follow their local paediatric empirical antibiotic guidelines. Clinicians elsewhere in Queensland should follow the Children’s Health Queensland paediatric antibiotic prescribing guidelines until the results of microbiological investigations are available.
Links
- Cairns (access via QH intranet)
- Townsville [PDF] (access via QH intranet)
- Gold Coast
- Children’s Health Queensland
Other treatments
There is no evidence to support the use of antihistamines or decongestants.14
Escalation and advice outside of ED
Clinicians can contact the services below if escalation of care outside of senior clinicians within the ED is needed, as per local practices. Transfer is recommended if the child requires a higher level of care.
| Advice may be required for the following children: |
|---|
|
| Reason for contact | Who to contact |
|---|---|
| Advice (including management, disposition or follow-up) | Follow local practice. Options:
|
| Referral | First point of call is the onsite/local paediatric service |
Disposition
Most children with isolated AOM without systemic illness can be discharged home.
On discharge provide the parent with:
- prescription for antibiotics (if needed)
- advice regarding the management at home (including analgesia, taking care not to get water in ear if perforation) and criteria for medical review (see Acute otitis media factsheet)
Follow-up
- with GP in 24-48 hours or up to 10 days depending on the management option chosen and the severity of the symptoms.
All children with a perforation should be reviewed by a GP to ensure it has healed (usually around 10 days).
All children with AOM should be seen by their GP at three months to ensure the effusion has resolved.
Referral to ENT specialist may be considered for children who meet the following criteria:
- effusion or perforation for more than 6 weeks
- hearing impairment for more than 6 weeks
- premature
- Indigenous or Torres Strait Islander background
Aeroplane travel
Parents frequently present to the ED to have their child with AOM assessed before flying. Airlines recommend against flying if the passenger is unable to clear their eustachian tubes. This is difficult to assess in younger children. Recommendations for young children are based on expert opinion in the absence of evidence. Children should be safe to fly two weeks after an adequately treated AOM, however many clinicians recommend waiting only 48 hours. These children should be given a nasal decongestant at least 30 minutes prior to take-off and landing and analgesia prior to flying.16 During take-off and landing they can be encouraged to suck, chew or swallow or, if old enough, perform a Valsalva manoeuvre to help equalise pressure.
Related documents
Guidelines
Factsheets
-
- American Academy of Pediatrics — Subcommittee on Management of Acute Otitis Media. (2013), ‘Diagnosis and management of acute otitis media’, Pediatrics, Vol. 113 (5): pp.1451-1465.
- Rothman, R., Owens, T., Simel, D.L. (2003), ‘Does this child have acute otitis media?’, Journal of the American Medical Association, Vol. 290 (12): pp. 1633-1640.
- Ruuskanen, O., Heikkinen, T. Otitis media: etiology and diagnosis. Pediatric Infectious Diseases Journal, 1994;13 (1 suppl 1):S23-S26 (microbial)
- Marom, T. et al. Viral-Bacterial Interactions in Acute Otitis Media Current Allergy and Asthma Reports December 2012, 12 (6) 551-558
- Bluestone, C., Klein, J. Otitis Media in Infants and Children. 3rd ed. New York, NY: WB Saunders; 2001
- Ruohola, A. Meurman, O. et al. Microbiology of acute otitis media in children with tympanostomy tubes: prevalence of bacteria and viruses. Clin Infect Dis 2006;43:1417-22
- Brennan-Jones, CG., Whitehouse, AJ, et al. Prevalence and risk factors for parent-reported recurrent otitis media during early childhood in the Western Australia Pregnancy Cohort (Raine) Study. Journal Paediatrics and Child Health 2015 Apr 51(4) 403-9.
- Salah, M., Abdel-Aziz, M et al. Recurrent acute otitis media in infants: analysis of risk factors. International Journal of Pediatric Otorhinolaryngology 2013; 77(10): 1665-9
- Liese, JG., Silfverdal, SA. Et al. Incidence and clinical presentation of acute otitis media in children aged <6 years in European medical practices. Epidemiology and Infection, 2014. 142.8: 1778-88.
- Berger, G. Nature of spontaneous tympanic membrane perforation in acute otitis media in children. J Laryngol Otol 1989; 103:1150-1153.
- Rosenfeld, RM., and Kay, D. Natural history of untreated otitis media. Laryngoscope 2003; 113(10), 1645-57.
- UpToDate in Pediatrics. Holding a child to minimise movement during an exam. [internet].Available from: http://www.uptodate.com/contents/acute-otitis-media-in-children-diagnosis?source=search_result&search=otitis%2Bmedia%2Bchildren&selectedTitle=2%7E150
- Tintinalli, J.E., Stapczynski, J.S., Ma, O.J., Cline, D.M., Cydulka, R.K., Meckler, G.D., (2011), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed McGraw-Hill]
- Leskinen, K. Complications of acute otitis media in children. Current Allergy and Asthma Reports, 2005; 5:308- 12.
- Venekamp RP, Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane Database of Systematic Reviews 2015, Issue 6. Art. No.: CD000219.DOI: 10.1002/14651858.CD000219.pub4
- Canadian Paediatric Society. Air travel and children’s health issues. Paediatrics and Child Health, 2007. Jan; 12(1): 45-50
-
Document ID: CHQ-GDL-60000
Version number: 4.0
Supersedes: 3.0
Approval date: 11/08/2022
Effective date: 11/08/2022
Review date: 11/08/2026
Executive sponsor: Executive Director Medical Services
Author/custodian: Queensland Emergency Care Children Working Group
Applicable to: Queensland Health medical and nursing staff
Document source: Internal (QHEPS) + External
Authorisation: Executive Director Clinical Services
Keywords: AOM, Otitis, media, middle ear, infection, 00710, paediatric, children, emergency, guideline,60000, antimicrobial stewardhsip
Accreditation references: NSQHS Standards (1-8): 1, 4, 8
-
This guideline is intended as a guide and provided for information purposes only. View full disclaimer.
Last updated: March 2024